Anxiety Disorders |
| Anxiety disorders are a group of mental disorders characterized by intense and persistent anxiety or fear, exceeding the normal stress of everyday life. These disorders affect a person's thinking, behavior, and physical health. The main anxiety disorders include: |
|
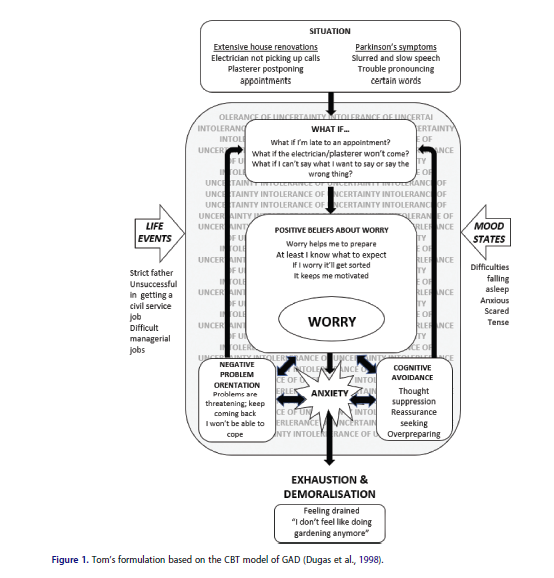
1. Generalized Anxiety Disorder (GAD) GAD is characterized by excessive and persistent worry and anxiety about various situations or events, which are difficult to control. Individuals with GAD constantly worry about health, finances, work, or other daily situations and often experience physical symptoms such as muscle tension, rapid heart rate, and insomnia. Read more |
|
a. Excessive Worry b. Dysfunctional Beliefs about Worry: c. Cognitive Biases: d. Emotional Avoidance: e. Reduced Tolerance for Uncertainty: f. Use of Safety Behaviors: Summary Diagram of the Cognitive Model of GAD
Initial Worry/Trigger → Dysfunctional Beliefs about Worry → Excessive Worry → Emotional Avoidance/Low Tolerance for Uncertainty → Safety Behaviors → Reinforcement of Worry and Maintenance of Anxiety This cognitive model illustrates how Generalized Anxiety Disorder (GAD) is maintained through a vicious cycle of negative thoughts, worry, and avoidance, which ultimately reinforces anxiety and reduces the individual’s ability to function normally. Cognitive Behavioral Therapy (CBT) focuses on breaking this cycle by changing dysfunctional thoughts and behaviors. Cognitive Behavioral Therapy and Anxiety Disorders Cognitive Behavioral Therapy (CBT) is considered one of the most effective treatments for Generalized Anxiety Disorder (GAD). Meta-analyses that examine the efficacy of CBT for GAD consolidate findings from various studies to determine its overall effect in reducing anxiety and improving the quality of life for individuals suffering from the disorder. Key Findings from Meta-Analyses on CBT for GAD:
Moderate Acceptance and Compliance Rates: Despite the proven benefits of CBT, some meta-analyses highlight moderate rates of patient acceptance and compliance, especially in the case of long-term therapy. This indicates the need for continuous monitoring and adjustment of treatment to ensure long-lasting results.
Overall Assessment: Meta-analyses confirm that CBT is one of the most effective treatments for GAD, offering significant benefits in reducing anxiety, improving co-occurring depression symptoms, and achieving long-term positive outcomes. However, its effectiveness depends on individual compliance and the adaptation of the therapy to each patient's specific needs. |
|
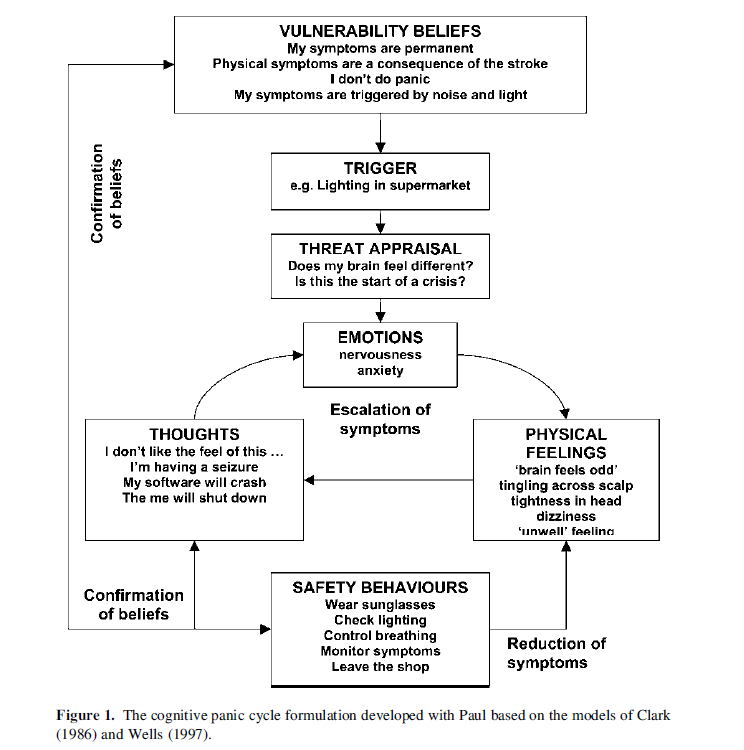
2. Panic Disorder It involves recurring panic attacks, which are sudden episodes of intense fear or discomfort, accompanied by physical symptoms such as rapid heartbeat, difficulty breathing, sweating, trembling, and a feeling of losing control. The individual may develop agoraphobia, which is the fear of being in places where escape would be difficult in the event of a panic attack. Learn more |
|
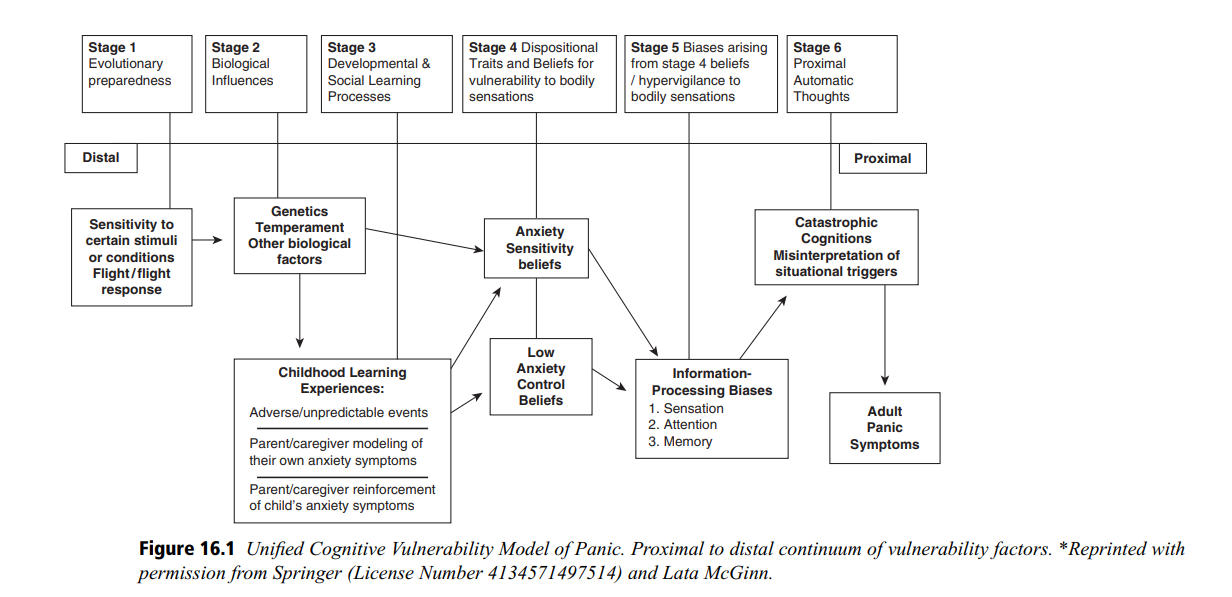
The Cognitive Model of Panic Disorder is a framework that explains how thoughts, emotions, physical reactions, and behaviors interact with one another and maintain the symptoms of panic disorder. This model is useful in therapy, especially in Cognitive Behavioral Therapy (CBT), as it helps patients understand how negative thoughts and interpretations can lead to panic attacks and worsen the issue. Let's explore the key components of the model in detail: a. Triggers Triggers can be internal (like physical sensations) or external (such as a stressful event). For example, a racing heartbeat or a feeling of dizziness can trigger a panic attack. b. Physical Symptoms These symptoms include rapid heartbeat, sweating, shortness of breath, dizziness, and a feeling of choking. While these are normal physical reactions, the patient may interpret them as threatening. c. Cognitive Interpretations Physical sensations are often interpreted catastrophically. For example, a racing heartbeat may be interpreted as "I'm having a heart attack" or "I'm losing control." These negative thoughts increase anxiety. d. Increased Anxiety Catastrophic thoughts lead to heightened anxiety and tension, which in turn intensifies physical symptoms. e. Behavioral Reactions Patients typically engage in avoidance behaviors (e.g., avoiding certain places or situations) or safety behaviors (e.g., carrying medications or always being accompanied by others), which perpetuate the panic cycle. f. Panic Cycle All these elements interact, creating a vicious cycle. Avoidance and safety behaviors prevent the patient from confronting and re-evaluating negative interpretations, thus maintaining panic. Cognitive Management Model In therapy, this model is used to:
Meta-Analyses Demonstrating the Effectiveness of CBT:
Several meta-analyses, such as the one by Mitte (2005), show that Cognitive Behavioral Therapy (CBT) effectively reduces the frequency and intensity of panic attacks, as well as associated symptoms of anxiety and depression. Patients participating in CBT experience significant improvement compared to control groups or placebo treatments.
Research indicates that the benefits of CBT are long-lasting. A meta-analysis by Hofmann et al. (2012) highlights that the positive effects remain for months or even years after the therapy ends, making it a sustainable therapeutic option.
Studies, such as the one by Cuijpers et al. (2016), reveal that CBT is as effective or even more effective than antidepressant medication, with fewer side effects and higher patient acceptance.
Research supports that CBT can be effective not only in individual sessions but also in group settings or even online, increasing the accessibility of the therapy. Meta-Analyses not supporting the effectiveness of CBT:
Conclusion: CBT is an effective therapeutic approach for panic disorder, with strong scientific evidence supporting its use. However, studies indicate that it is not a cure-all, and its success may depend on the patient, comorbidities, and other factors. Personalizing the therapy and continuously evaluating its effectiveness are crucial for optimal outcomes. |
|
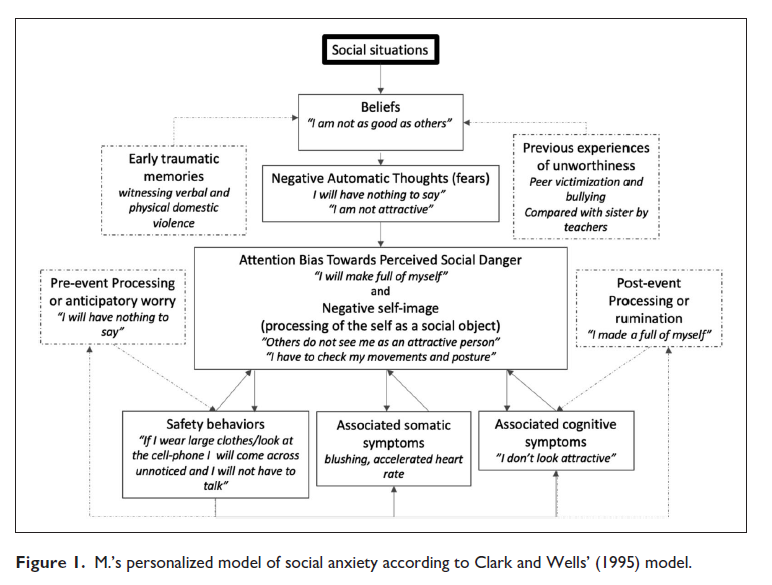
3. Social Anxiety Disorder (Social Phobia): This disorder manifests as an intense fear or anxiety in social situations where the individual might be judged by others. The person fears criticism, rejection, or embarrassment, which may lead them to avoid social interactions, public speaking, or other situations where they feel exposed to the attention or evaluation of others. Learn more |
This model helps patients break the cycle of social phobia and improve their quality of life by addressing and modifying dysfunctional perceptions and behaviors. The effectiveness of Cognitive Behavioral Therapy (CBT) for social phobia (social anxiety disorder) has been extensively researched through numerous studies and meta-analyses. These analyses compile data from various studies to provide a comprehensive overview of the therapy's effectiveness. While CBT is generally considered one of the most effective treatments for social phobia, there are also findings that indicate challenges and limitations. Below is a summary of meta-analyses that support and question the effectiveness of CBT. Meta-Analyses Demonstrating the Effectiveness of CBT for Social Phobia
Conclusion Cognitive Behavioral Therapy (CBT) is widely recognized as one of the most effective treatments for social phobia, with numerous meta-analyses supporting its use. However, its effectiveness may vary depending on the patient and comorbid conditions, and it is not always superior to other therapies or placebo treatments. Personalization of therapy and ongoing assessment of effectiveness are crucial for the optimal management of social phobia. |
|
4. Obsessive-Compulsive Disorder (OCD) This disorder is characterized by unwanted and recurring thoughts (obsessions) and/or compulsive behaviors that the individual feels driven to perform to reduce anxiety or prevent a perceived danger. These obsessions and compulsions are time-consuming and interfere with daily life. Learn more |
|
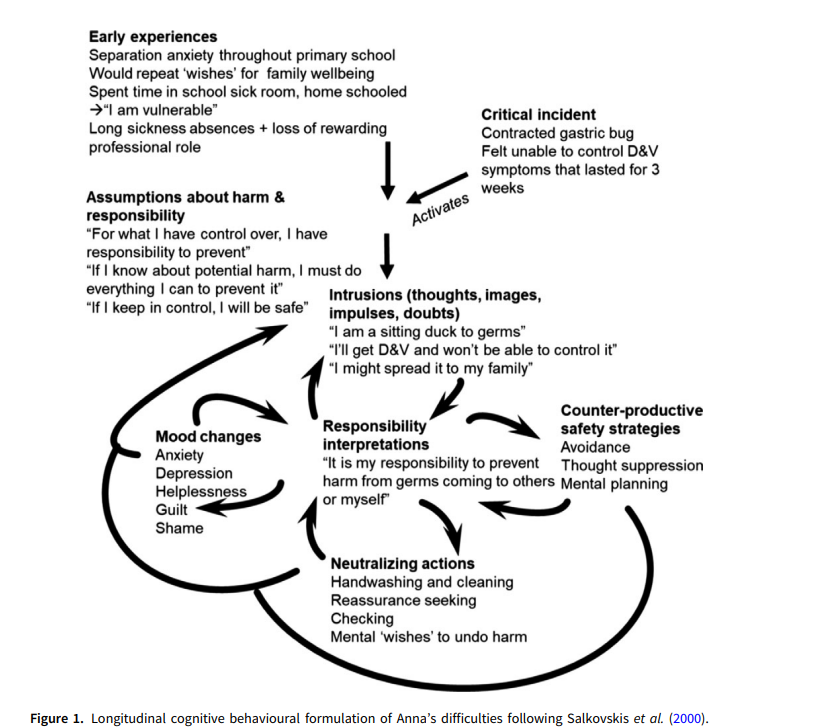
The cognitive model of Obsessive-Compulsive Disorder (OCD) according to Salkovskis (2000) is one of the most well-known approaches in Cognitive Behavioral Therapy (CBT) for understanding and treating the disorder. Salkovskis developed a model that explains how dysfunctional beliefs and cognitive processes maintain and exacerbate OCD symptoms. Analysis of Salkovskis' (2000) Cognitive Model of OCD a. Triggering Stimuli External events or internal thoughts that provoke intrusive thoughts, such as seeing a dirty object, having a thought about potential harm, or experiencing an impulsive idea. b. Intrusive Thoughts These thoughts intrude frequently and occur in everyone, but for individuals with OCD, they take on significant meaning. An example of an intrusive thought is: "If I don't turn off the stove properly, a fire could start and cause destruction." c. Dysfunctional Interpretations of Thoughts Patients often view their intrusive thoughts as highly significant, threatening, or reflective of their character. Instead of ignoring them, they believe these thoughts imply something terrifying or indicate that they are bad or dangerous people. For example, the thought "If I thought about harming someone, it means I want to or will do it." d. Negative Emotional Reactions Dysfunctional interpretations lead to intense negative emotions such as anxiety, shame, guilt, and fear. These emotions reinforce the perception that the thoughts are dangerous or revealing. e. Responsibility and Threat Overestimation Individuals with OCD often feel excessive responsibility and overestimate the likelihood and severity of a negative outcome. They believe they must take action to prevent a supposed disaster. f. Compulsive Behaviors As a result of the negative emotions, individuals resort to compulsive behaviors or mental acts (e.g., repetitive checking, handwashing, counting) to reduce anxiety or prevent the perceived harm. These behaviors temporarily alleviate anxiety but strengthen the belief that intrusive thoughts are dangerous and that compulsive actions are necessary. g. Maintenance of the OCD Cycle Compulsive behaviors prevent individuals from learning that intrusive thoughts are harmless and that the supposed harm will not occur. Thus, the thoughts continue to provoke anxiety, and the need for compulsive actions remains. Summary of the Vicious Cycle: Intrusive Thoughts → Dysfunctional Interpretations → Anxiety → Compulsive Behaviors → Temporary Relief → Reinforcement of Intrusive Thoughts. Cognitive Intervention and Treatment: Challenging Dysfunctional Beliefs: The therapist assists the individual in recognizing and questioning exaggerated estimates of responsibility and threat. Exposure and Response Prevention (ERP): The individual is deliberately exposed to feared situations without resorting to compulsive behaviors. Training in Relaxation and Anxiety Management Techniques: This helps reduce anxiety stemming from intrusive thoughts. The cognitive model proposed by Salkovskis provides a clear understanding of how thoughts and behaviors interact to maintain OCD and serves as a foundation for effective therapeutic intervention. The effectiveness of Cognitive Behavioral Therapy (CBT) for Obsessive-Compulsive Disorder (OCD) has been extensively examined through numerous studies and meta-analyses. These meta-analyses offer a comprehensive view by aggregating and evaluating data from various studies to determine the extent to which CBT is effective in treating OCD. While there is strong evidence supporting the efficacy of CBT, some reservations and limitations have been identified. Below is a summary of the meta-analyses that support and challenge the effectiveness of CBT for OCD: Meta-Analyses Demonstrating the Effectiveness of CBT for OCD
Conclusion: Cognitive Behavioral Therapy (CBT), particularly the Exposure and Response Prevention (ERP) approach, is widely recognized as one of the most effective therapeutic methods for Obsessive-Compulsive Disorder (OCD). However, its effectiveness may vary depending on the individual patient, the severity of symptoms, and the quality of the therapeutic relationship. Despite its proven efficacy, challenges remain that necessitate further research and tailored interventions to enhance treatment outcomes and ensure the long-term maintenance of positive changes. |

|
5. Specific Phobias Specific phobias involve intense fear or anxiety regarding a particular object or situation (e.g., heights, spiders, flying, injections). The individual systematically avoids the stimulus that triggers fear, and this avoidance can significantly limit daily functioning. Learn more |
|
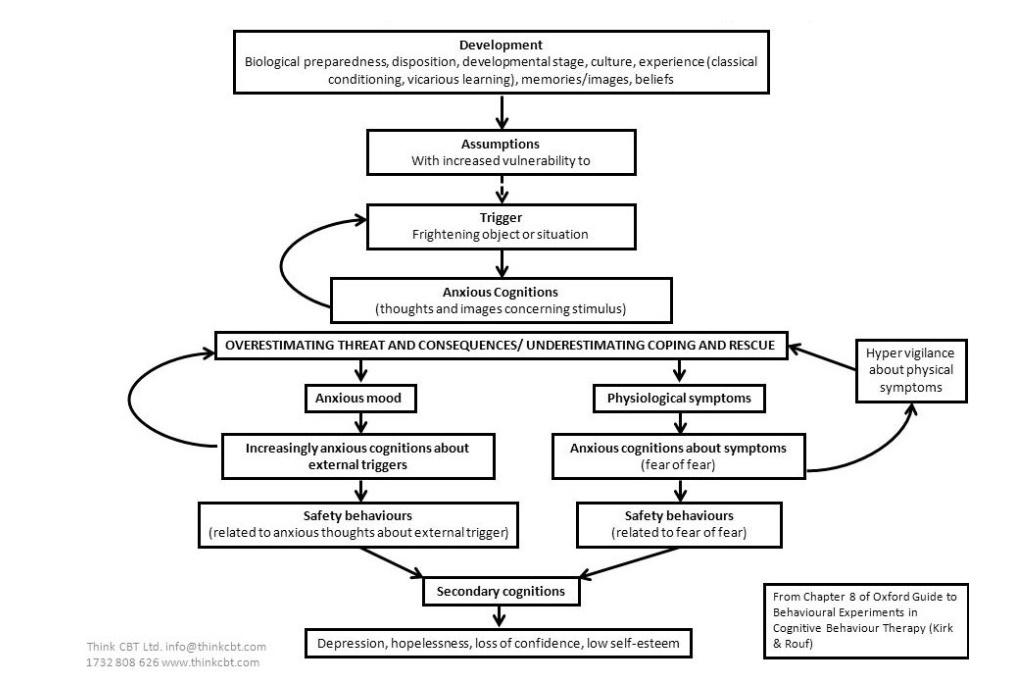
External events or situations that provoke intense fear. For example, a person with a phobia of snakes may feel fear when seeing a snake in a picture or in real life. b. Automatic Negative Thoughts Thoughts that arise immediately and automatically when the person is exposed to the phobic object or situation. These thoughts are typically catastrophic and exaggerated, such as "It will bite me," "I will die," or "I won't be able to handle it." c. Dysfunctional Beliefs and Cognitive Distortions Individuals tend to overestimate the likelihood of a dangerous situation and the severity of its consequences. These beliefs may involve an exaggerated perception of threat and the belief that they are unable to cope with the situation. For instance, someone may believe that if they board an airplane, it will crash. d. Physiological Anxiety Responses Exposure to the phobic stimulus triggers intense physical reactions, such as rapid heartbeat, sweating, trembling, dizziness, and difficulty breathing. These responses reinforce the belief that the situation is dangerous and threatening. e. Avoidance Behaviors To reduce anxiety, individuals systematically avoid exposure to the phobic object or situation. For example, a person with a fear of flying may avoid traveling by airplane, even if this causes significant difficulties in their life. f. Short-term Relief and Maintenance of Phobia Avoidance provides temporary relief from anxiety but reinforces the belief that the phobic object is dangerous in the long term. The individual never gives themselves the opportunity to learn that their fear is exaggerated or unfounded. g. Reinforcement of Negative Beliefs The success of avoidance reinforces the belief that the person did the right thing to protect themselves. However, this reinforcement contributes to the maintenance of the phobia, as the individual never learns to confront the source of their fear. The Vicious Cycle of Specific Phobia: Trigger → Automatic Negative Thoughts → Physiological Anxiety Responses → Avoidance → Short-term Relief → Reinforcement of Phobia. Cognitive Interventions and Treatment:
The cognitive diagram by Kirk and Rouf provides a comprehensive framework for understanding specific phobias and illustrates how dysfunctional thoughts and avoidance behaviors maintain anxiety, while cognitive restructuring and exposure are keys to effective treatment. Cognitive Behavioral Therapy (CBT) has been extensively studied for treating specific phobias, such as fears of animals, heights, flying, and injections. Meta-analyses provide clear evidence for the effectiveness of CBT but also highlight some limitations. Below is a summary of meta-analyses that support and question the effectiveness of CBT for specific phobias. Meta-Analyses Demonstrating the Effectiveness of CBT for Specific Phobias
Conclusion: |
|
6. Post-Traumatic Stress Disorder (PTSD) PTSD is triggered by exposure to a traumatic event, such as war, natural disasters, or sexual assault. Individuals with PTSD experience recurrent memories of the event, nightmares, avoidance of stimuli that remind them of the trauma, and heightened irritability or anxiety. Learn More |
|
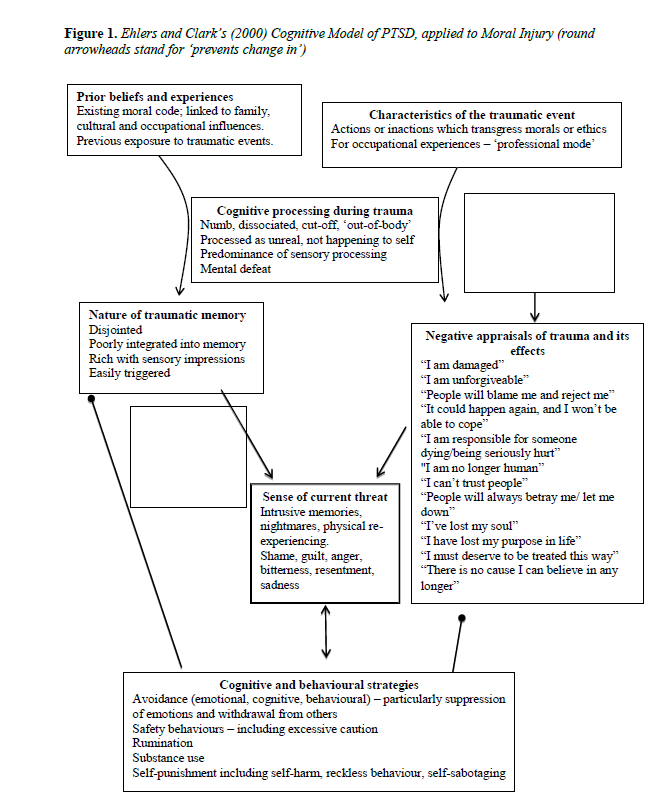
Individuals process the traumatic event in a way that reinforces the perception that the world is dangerous and that they are incapable of handling future threats. This includes overly negative interpretations of the events, such as "I was completely powerless" or "I can't get over this." b. Dysfunctional Beliefs about Self and the World: Beliefs developed after the trauma may include negative thoughts about oneself ("I am weak"), about others ("People are not trustworthy"), and about the future ("I will never be safe again"). These beliefs contribute to the ongoing sense of threat and helplessness. c. Heightened Sense of Threat: Constant vigilance and focus on danger cues enhance the feeling that the individual is always at risk. This state of hyper-vigilance intensifies anxiety symptoms and contributes to trauma re-experiencing (flashbacks). d. Fragmented and Disorganized Recall of the Trauma: Traumatic memories are often fragmented and not properly integrated into autobiographical memory, rendering them dysfunctional and easily triggered. The individual may experience the events as if they are occurring in the present. e. Avoidance and Safety Strategies: Individuals adopt avoidance behaviors (e.g., avoiding situations that remind them of the trauma) and safety strategies (e.g., hyper-vigilance), which provide temporary relief from anxiety but hinder the processing of traumatic experiences. These strategies reinforce the maintenance of PTSD and increase the individual's dysfunctionality. f. Symptom Triggers: Everyday stimuli associated with the trauma, such as sounds, images, or even specific thoughts, can trigger memories and symptoms. These triggers are not always apparent to the individual, resulting in unexpected outbursts of anxiety or panic. g. Vicious Cycle of Symptom Reinforcement: The individual remains "trapped" in a cycle of re-experiencing, hyper-vigilance, and avoidance, which continuously reinforces feelings of fear and helplessness. This cycle sustains PTSD and prevents normal recovery. Diagram of the Model: Traumatic Event → Leads to dysfunctional processing and fragmented memories. Negative Processing and Beliefs → Reinforce the sense of constant threat and helplessness. Increased Hyper-Vigilance and Avoidance → Sustain symptoms through strategies that hinder memory processing. Triggers and Re-experiencing → Cause the re-emergence of symptoms. Maintenance of the Sense of Threat → Enhances dysfunctional beliefs and increases distress. Therapeutic Interventions:
|
|
7. Agoraphobia Agoraphobia is the fear or anxiety of being in situations where escape might be difficult, or help may not be readily available in the event of a panic attack or other problem. This can include fears of being outside the home, in crowds, on public transportation, or in similar situations. Learn More |
|
Agoraphobia often begins after one or more panic attacks occur in a public space. The individual may develop an intense fear of experiencing another panic attack in similar situations. b. Dysfunctional Thoughts and Perceptions: The individual starts to develop catastrophic thoughts about the possibility of having a new panic attack and its consequences. These thoughts may include fears such as, “If I have a panic attack, I won’t be able to escape,” or “If I faint, no one will help me.” These thoughts are excessively catastrophic and often do not correspond to reality, yet they create intense fear and anxiety. c. Avoidance and Safety Behaviors: Due to dysfunctional thoughts, the individual begins to avoid situations they believe may trigger anxiety or lead to a panic attack (e.g., crowded places, public transport, open spaces). Additionally, the individual may develop safety behaviors, such as carrying medications, insisting on being accompanied by others, or seeking nearby exits. d. Maintenance of Fear and Reinforcement of Avoidance: Avoidance and safety behaviors prevent the individual from learning that their fears are exaggerated or unfounded. This creates a vicious cycle where avoidance reinforces the fear and the belief that situations are truly dangerous. e. Reinforcement of Agoraphobia: Fear and avoidance lead to a significant reduction in quality of life, as the individual increasingly limits their activities. This social withdrawal and isolation can further reinforce agoraphobia, making the disorder even more difficult to treat. Interventions Based on the Cognitive Model The treatment of agoraphobia through Cognitive Behavioral Therapy (CBT) aims to achieve the following:
Meta-Analyses Not Supporting the Effectiveness of CBT for Agoraphobia
Some meta-analyses, such as that by Craske and Barlow (2001), have shown that while CBT is effective in the short term, long-term outcomes are not always as positive. In certain cases, symptoms of agoraphobia may return a few months after treatment, especially if adequate exposure practice has not been undertaken or if the individual does not continue to apply the techniques learned during therapy.
Another controversial aspect is that some meta-analyses (e.g., Benish et al., 2008) suggest that CBT does not significantly outperform other psychological treatments for agoraphobia, such as supportive psychotherapy or pharmacotherapy. While CBT is effective, it does not appear to excel significantly over these other approaches in all cases.
Some studies indicate that the effectiveness of CBT may be influenced by the severity of the disorder, the personal characteristics of the patient, and adherence to therapeutic guidelines. For instance, Tolin et al. (2006) argued that CBT might be less effective for patients with severe comorbid disorders, such as depression or social phobia, which could hinder the full application of the therapeutic techniques. Conclusion Most meta-analyses support the effectiveness of Cognitive Behavioral Therapy (CBT) for agoraphobia, particularly concerning the reduction of anxiety symptoms and the avoidance of panic attacks. However, there is skepticism about the long-term effectiveness in certain cases and about whether it significantly surpasses other therapies. Overall, CBT remains one of the most documented and widely used treatments for agoraphobia, although it is essential to tailor it to the individual needs of the patient.
|
|
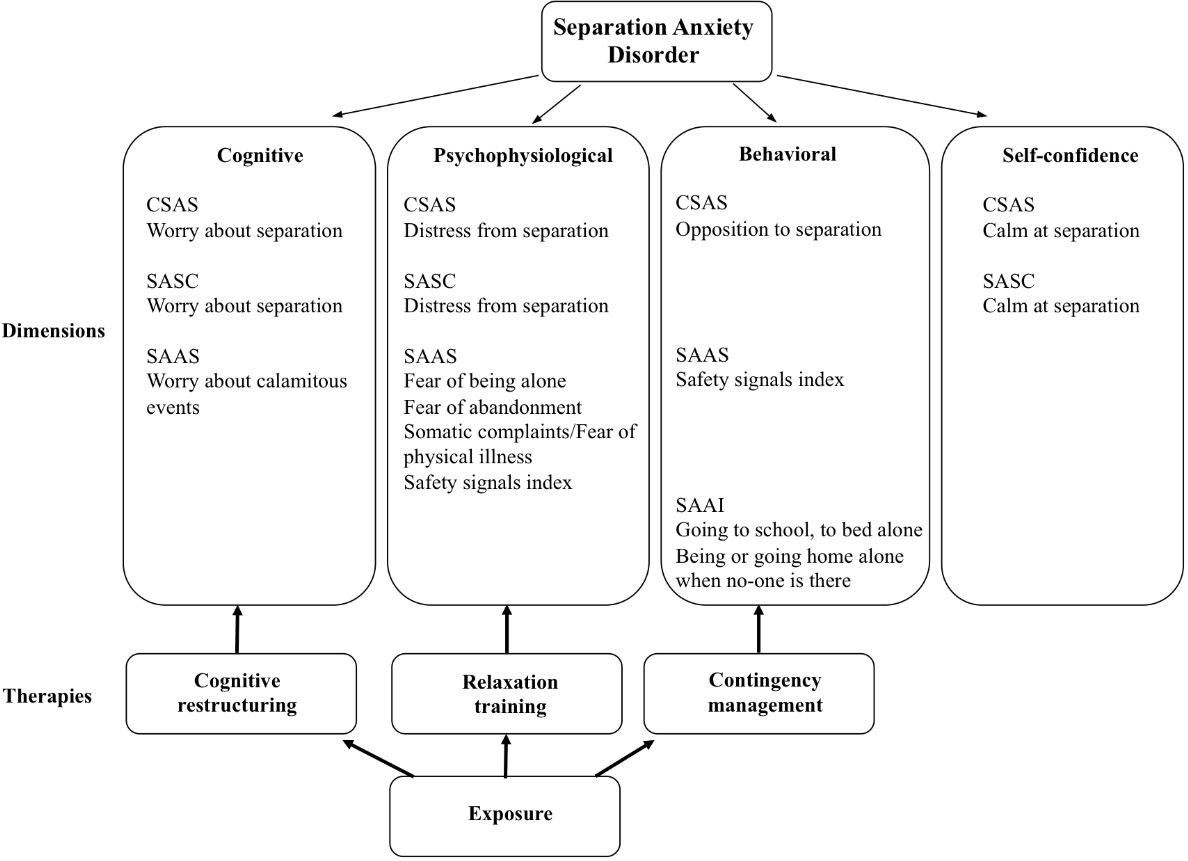
8. Separation Anxiety Disorder This disorder involves intense anxiety or fear when an individual is separated from a person with whom they have a strong emotional bond, such as a parent or partner. It is more common in children but can also occur in adults. Learn More |
Most meta-analyses support that Cognitive Behavioral Therapy (CBT) is an effective approach for treating separation anxiety, particularly when combined with parental involvement and training. However, some studies highlight certain limitations, such as the comparatively small difference in effectiveness compared to other therapeutic approaches and the inconsistency in long-term results, especially in severe cases. Overall, CBT remains one of the most well-documented and widely used treatments for separation anxiety, but its application should be tailored to the individual’s needs.
|
|
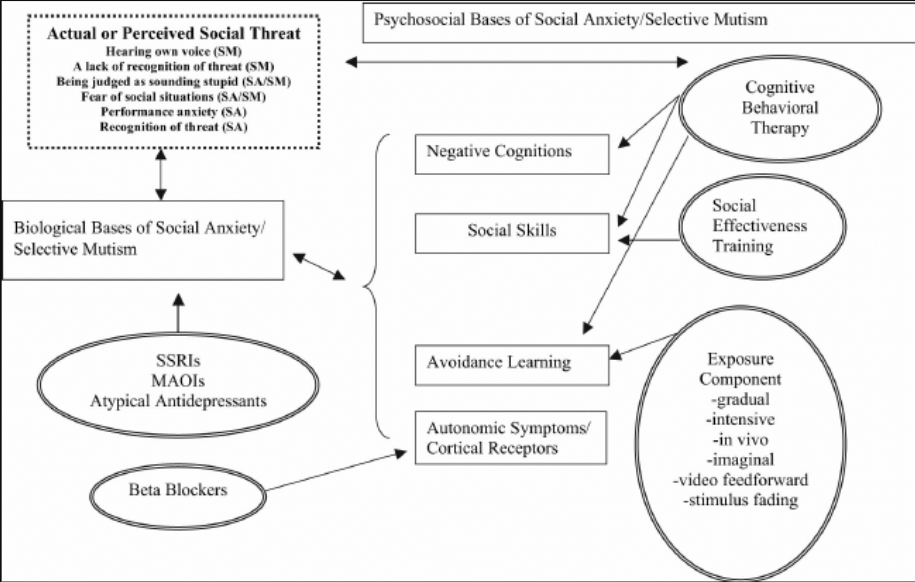
9. Selective Mutism Selective mutism is an anxiety disorder that typically manifests in childhood, where the child is unable to speak in specific social situations (e.g., at school), despite being able to communicate normally in other settings (e.g., at home with family). These disorders can vary in intensity and impact daily life, but all significantly affect the individual’s life and psychological well-being. Treatment may include cognitive-behavioral therapy, medication, or a combination of both. Learn more |
|
Key Elements of the Cognitive Model for Selective Mutism
a. Dysfunctional Thoughts (Cognitions): Children with selective mutism often harbor destructive and dysfunctional thoughts regarding speaking in specific social situations. These thoughts may include fears of negative judgment from others, the belief that they will say something wrong, or the concern of being ridiculed. Examples of such thoughts include: "If I speak, they will laugh at me" or "It's better to stay silent so I don't say something wrong." b. Emotional Reactions (Emotions): These dysfunctional thoughts lead to intense negative emotions such as anxiety, fear, or panic when the child finds themselves in situations where speaking is expected. The anxiety can be so overwhelming that it prevents the child from uttering even a single word. Additionally, the individual may experience physical symptoms of anxiety, such as trembling, sweating, or stomachaches when in social situations where speaking is anticipated. c. Avoidance and Silence as Behavior (Behavior): To evade the anxiety associated with speaking, children with selective mutism choose to remain silent in fear-inducing situations. Avoiding speech becomes a protective behavior that temporarily reduces anxiety but, in the long term, sustains and reinforces the disorder. The child may also resort to non-verbal means of communication, such as nodding or gesturing, to avoid the necessity of speaking. d. Reinforcement and Maintenance of the Problem: The avoidance of speaking and the silence reinforce the initial dysfunctional thoughts, as the child misses the opportunity to realize that their fears are exaggerated or unfounded. For instance, by remaining silent, the child does not give themselves the chance to see that they can speak without experiencing the negative consequences they dread. Parents or teachers may inadvertently reinforce the silence by showing excessive understanding and allowing avoidance or by trying to "force" the child to speak, which can heighten the anxiety. Interventions Based on the Cognitive Model Cognitive Behavioral Therapy (CBT) for selective mutism focuses on the following:
The cognitive model for selective mutism explains how catastrophic thoughts, anxiety, and silence interconnect and sustain this disorder. Cognitive Behavioral Therapy (CBT) offers effective strategies for addressing selective mutism by focusing on modifying dysfunctional thoughts, gradual exposure to anxiety-inducing situations, and training caregivers. Through these interventions, children can develop the confidence and skills necessary to speak comfortably in all social situations.
Effectiveness of Cognitive Behavioral Therapy (CBT) for Selective Mutism The effectiveness of Cognitive Behavioral Therapy (CBT) for selective mutism has been examined through various studies and meta-analyses, providing a comprehensive overview of the outcomes associated with this therapeutic approach. Here is a summary of findings from meta-analyses that demonstrate the effectiveness of CBT and those that highlight limitations or controversial results. Meta-analyses Demonstrating the Effectiveness of CBT for Selective Mutism
Most meta-analyses support the view that Cognitive Behavioral Therapy (CBT) is effective for treating selective mutism, especially when applied in conjunction with other therapeutic approaches and with parental involvement. However, there are reports highlighting limitations, such as reduced effectiveness in severe cases or different contexts, as well as limited superiority compared to other therapies. Overall, CBT is considered a significant and evidence-based therapeutic option for selective mutism, but its application should be tailored to the individual needs and circumstances of each child.
|